Select your language
")
")
Glaucoma

Glaucoma
There are several types of glaucoma, but they mainly fall into two groups of open and closed angle glaucoma.
1] Open angle glaucoma
This is also called chronic glaucoma and is the most frequent type. Fluid produced within the eye drains out of a fine network of channels. As one gets older these channels become less good at draining away the fluid and so the pressure can build up within the eye. A sustained rise in pressure can damage the Optic Nerve and this can cause a disturbance in the visual field and sharpness of vision – this we call glaucoma.
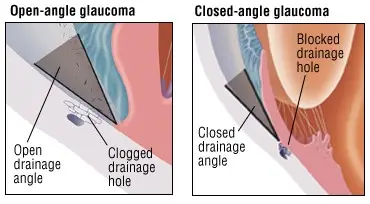
2] Angle closure glaucoma
This is also called acute glaucoma. If the draining channels of the eye suddenly block off there is a sharp rise in pressure which can be very painful and cause sight loss. It is an emergency and you should seek immediate attention.
Normal tension glaucoma
Sometimes the pressure in the eye is ‘normal’ (below 21mmHg), but you can still have glaucoma. This is because only part of the damage to the optic nerve is due to pressure. The other part is due to reduced blood supply to the eye. Strictly it is not a separate type of glaucoma, but really an open angle glaucoma which is less dependent on pressure within the eye.
Ocular hypertension
Ocular hypertension is when the pressure of the eye is raised but there is no damage done to the optic nerve. Close monitoring is all that is needed but occasionally you may be offered eye drops to bring your pressure into a safer zone.
Symptoms of glaucoma
With open angle glaucoma often there are no symptoms as the damage to the optic nerve is so slow you do not notice it. Only when it is established you notice a disturbance of visual field and acuity. Acute glaucoma is very different and produces a painful red eye with reduced acuity. Some people also feel sick, faint and vomit. Coloured rings around lights in dim illumination can be a warning sign of this type of glaucoma. People who are in their 60s and longsighted are most at risk.
Risk factors of open angle glaucoma:
- Increasing incidence over the age of 40
- African origin – greater risk
- Genetic – you should have regular eye tests from the age of 35 if there is a close relative with glaucoma
- Short sight (Myopia) – greater risk
- Diabetes – greater risk
Diagnosis
This is made by your Ophthalmologist who will check the pressure within your eye, look at the optic nerve and plot your visual field.
Treatment
The aim is to make the pressure in the eye lower. This can be done with eye drops, laser or surgery.
A] Eye drops
The most frequently used are:
- Timoptol – a beta blocker which reduces the fluid production within the eye
- Xalatan / Lumigan / Travatan – prostaglandin analogues which reduce the fluid production as well as increasing the drainage
- Trusopt – a carbonic anhydrase inhibitor that reduces the fluid production within the eye
- Combinations of these drops for ease of use such as Xalacom, Ganfort, Cosopt
- Acetazolamide (Diamox) is like a tablet form of Trusopt and is good at rapidly reducing the pressure in the eye
B] Laser treatment
This can help open up the drainage system but has a very variable response between people and tends to wear off with time. It is performed as an outpatient.
C] Surgery (Trabeculectomy)
Much less surgery is done for glaucoma now due to the success of the modern eye drops available. Surgery is however still needed for complicated cases or where there is continuing damage to the optic nerve despite good medical treatment.
Prevention
All adults over the age of 40 should have eye tests every 2 years to check for the early signs of glaucoma.






